Ретроспективный анализ бремени лихорадки денге и тенденций назначения лекарственных препаратов в больницах третичного уровня города Махбубнагар, штат Телангана, за период с января 2019 г. по декабрь 2023 г.
Ретроспективный анализ бремени лихорадки денге и тенденций назначения лекарственных препаратов в больницах третичного уровня города Махбубнагар, штат Телангана, за период с января 2019 г. по декабрь 2023 г.

Аннотация
Обоснование и цели: Лихорадка денге — вирусное заболевание, передающееся москитами, которое представляет собой серьезную проблему для мирового здравоохранения. В последние годы Хайдарабад стал очагом инфекции денге, при этом в соседнем районе Махбубнагар также наблюдается рост распространенности заболевания. Данное исследование направлено на оценку демографического распределения, тяжести течения болезни и структуры назначения лекарственных препаратов в случаях лихорадки денге в Махбубнагаре, штат Телангана.
Методы: Было проведено многоцентровое ретроспективное исследование с использованием медицинских карт пациентов, листов назначений и лабораторных записей Медицинского колледжа и больницы S.V.S., а также Государственной больницы общего профиля в Махбубнагаре. Данные за период с января 2019 г. по декабрь 2023 г. были проанализированы с использованием методов описательной статистики и критерия хи-квадрат для оценки сезонных и годовых тенденций.
Результаты: Случаи денге чаще встречались среди мужчин (59,7%), лиц в возрасте ≤20 лет (48,3%) и сельских жителей (82,66%). Тяжелые случаи составили 64,66%, при этом 87% пациентов потребовалась госпитализация на срок ≥5 дней. Более чем у 42 пациентов количество тромбоцитов было <50 000. Наиболее часто назначаемыми средствами были жаропонижающие препараты (100%) и внутривенные вливания (97,1%), за которыми следовали противорвотные средства (79,4%). Препарат Карипилл (Caripill) использовался для поддержания уровня тромбоцитов в 68% случаев, а антимикробные препараты назначались более чем в 50% случаев.
Заключение: Отсутствие специфической противовирусной терапии лихорадки денге в сочетании с ростом ее распространенности подчеркивает необходимость повышения осведомленности населения, совершенствования мер профилактики и продолжения исследований эффективных стратегий лечения.
1. Introduction
Dengue is a vector-borne disease transmitted by Aedes mosquitoes, chiefly Ae. aegypti and Ae. albopictus, and caused by the dengue virus (DENV), a member of the Flaviviridae family. Approximately 4 billion individuals, representing over half of the global population, live in areas at risk of dengue transmission. Each year, nearly 400 million infections occur worldwide, of which about 100 million become symptomatic and nearly 40,000 result in death due to severe disease.
There are four antigenically distinct serotypes (DENV-1 to DENV-4), and individuals may experience multiple infections during their lifetime. Secondary infections may be aggravated by antibody-dependent enhancement (ADE), which increases the risk of severe manifestations such as dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS)
, , , .Hyderabad, the capital of Telangana, has recently emerged as a dengue hotspot. Mahabubnagar, a neighboring district located approximately 100 km away, has close geographical and socioeconomic connections with Hyderabad and experiences substantial population mobility between the two cities. Conditions in Mahabubnagar such as inadequate drainage infrastructure, intermittent water supply, rapid urbanization, and open drainage systems create favorable environments for mosquito breeding and dengue transmission.
Despite these risk factors, comprehensive data on dengue prevalence and prescribing trends specific to Mahabubnagar remain limited. Understanding the local disease burden, demographic patterns, and treatment practices is therefore important for effective public health planning. This study presents a retrospective analysis of clinical characteristics and prescribing patterns of dengue in Mahabubnagar over a five-year period, incorporating severity scoring, rural disease burden, and data from two tertiary care hospitals.
The prevalence of dengue increased in 2023 compared to 2022, with more than 2,972 cases reported in Telangana, India
. Recurrent outbreaks, associated co-infections, and the lack of specific antiviral therapy contribute significantly to the public health and economic burden of dengue. Since approximately 75% of dengue cases reported in Hyderabad originate from surrounding districts, including Mahabubnagar, evaluating the prevalence, severity, co-infections, demographics, and prescription patterns of dengue in this region is essential for district-level public health planning. The objectives of the present investigation are to determine the prevalence, demographic distribution, and clinical profile of hospitalized dengue patients in Mahabubnagar; to evaluate seasonal and year-wise disease severity; and to describe prescribing patterns associated with hospitalized dengue cases in Mahabubnagar (MBNR).2. Materials and methods
2.1. Study Design
This multicenter retrospective observational study analyzed hospitalized, laboratory-confirmed dengue cases to evaluate disease burden, demographic trends, clinical features, and prescribing patterns in Mahabubnagar, Telangana. The retrospective design enabled analysis of existing hospital records over a five-year period.
2.1.1. Study Setting and Duration
The study was conducted in two tertiary care hospitals in Mahabubnagar:
1. S.V.S. Medical College & Hospital, a teaching hospital serving urban and semi-urban populations.
2. Government General Hospital, Mahabubnagar, a public hospital primarily serving rural and low-income communities.
The study period extended from January 2019 to December 2023, and data collection was performed over six months after obtaining institutional permission and ethical approval (IEC/DHR-03/(03/03/2023/0543))
.Probable dengue fever: A case compatible with the clinical description of dengue during an outbreak or non-ELISA-based NS1 antigen/IgM positive.
Confirmed dengue fever: A case with clinical features of dengue and at least one of the following:
– isolation of dengue virus from serum, plasma, or leucocytes;
– IgM antibody detection by ELISA in a single serum sample;
– demonstration of dengue virus antigen by NS1-ELISA;
– IgG seroconversion or four-fold increase in paired sera;
– detection of viral nucleic acid by polymerase chain reaction (PCR).
2.1.2. Disease severity
Disease severity was assessed using the Dengue Severity Index Score (Surangrat/Pongpan et al., 2013), which incorporates clinical and laboratory parameters including bleeding, shock, and routine laboratory values. Patients were categorized as mild (2–4), moderate (5–7), or severe (8–9). Based on this scoring system, 73 patients (12,16%) were classified as mild, 139 (23,16%) as moderate, and 388 (64,66%) as severe dengue.
2.1.3. Inclusion Criteria
Hospitalized patients aged ≥1 year with confirmed dengue infection diagnosed by NS1 antigen, IgM serology, or both according to WHO criteria, and with complete medical records including laboratory and treatment data.
Exclusion Criteria:
– patients with unconfirmed or ambiguous diagnosis;
– incomplete records or discharge against medical advice;
– co-infections such as malaria, typhoid, or leptospirosis without isolated dengue confirmation.
2.2. Data Sources and Collection Procedure
Data were extracted using a structured proforma from patient case sheets, treatment charts, laboratory reports, and discharge summaries.
Collected variables included:
1. Demographics: age, gender, residence (rural/urban), occupation.
2. Clinical features: fever onset, symptoms, vital signs, comorbidities.
3. Laboratory findings: blood parameters, platelet count, liver function tests, NS1 antigen and IgM status.
4. Disease severity: categorized using WHO guidelines and Dengue Severity Index Score.
5. Treatment details: drug names, dose, route, supportive therapy (IV fluids, Caripill, antimicrobials).
6. Hospital stay duration.
2.2.1. Assessment of prescribing patterns
All medications documented in treatment charts and discharge summaries were recorded by drug name, frequency, route, and duration. Drugs were categorized into therapeutic classes including antipyretics, antiemetics, intravenous fluids, antimicrobials, platelet-supportive agents, and blood products. The number and percentage of patients receiving each drug class were calculated.
Among the 600 dengue cases, hematological data were available for 248 patients, while laboratory results were missing in 352 cases due to incomplete documentation in hospital records. Hematological analysis was therefore performed only for the available 248 cases using complete-case analysis, whereas demographic, clinical, and prescribing analyses included all 600 patients to maintain statistical power.
2.3. Statistical Analysis
Data were entered into Microsoft Excel 2019 (Microsoft Corp., Redmond, WA, USA) and verified for accuracy. Descriptive statistics including means, percentages, and ranges were used to summarize variables. The Chi-square (χ²) test was applied to evaluate the association between month of admission and year-wise dengue trends to identify seasonal patterns. A p-value <0,05 was considered statistically significant.
3. Results
Among the 600 patients analyzed, 358 (59,7%) were male and 242 (40,3%) were female. The highest number of cases (48,3%) occurred in individuals aged ≤20 years, followed by the 21–30 age group (26,5%). A large majority of patients (496 cases; 82,66%) were from rural areas, highlighting the disproportionate burden of dengue in underdeveloped settings.
Most infections occurred during the monsoon and post-monsoon months (September–November), coinciding with increased mosquito breeding in stagnant water. Seasonal analysis demonstrated a highly significant association between month and year of admission (χ² = 399,95, p <0,001), indicating a clear post-monsoon surge in dengue cases .
Patient demographics, dengue severity, and duration of hospital stay are presented in Table 1. The most common clinical complaints were fever, cough, generalized body pain, loose motions, vomiting, and abdominal pain. Rare symptoms included blood in stools (one patient), blurred vision with pedal edema (one patient), and tingling sensations in the limbs (seven patients). These chief complaints are provided in the 1st supplementary file.
Table 1 - Demographic characteristics and duration of hospital stay of patients
Characteristics | No of patients | Percentage | ||
Gender | ||||
FEMALE | 242 | 40,3 | ||
MALE | 358 | 59,7 | ||
Age in years | ||||
<= 20 | 290 | 48,3 | ||
21 – 30 | 144 | 24,0 | ||
31 – 40 | 78 | 13,0 | ||
41 – 50 | 46 | 7,7 | ||
51+ | 42 | 7,0 | ||
Total | 600 | 100,0 | ||
Mean ± SD : 23,87±14,96 | ||||
Geographical distribution | ||||
Rural | 496 | 82,66 | ||
Urban | 104 | 17,33 | ||
Total | 600 | 100 | ||
Severity of dengue infection | ||||
Types of scaling |
|
| ||
Mild (2–4) | 73 | 12,16 | ||
Moderate (5–7) | 139 | 23,16 | ||
Severe (8–9) | 388 | 64,66 | ||
Total | 600 | 100 | ||
Duration of hospital stay | ||||
No of days | No of patients | Percentage | ||
≥5 | 522 | 87% | ||
<5 | 78 | 13% | ||
Total | 600 | 100% | ||
Serological diagnosis showed that 212 patients were NS1 antigen positive, 155 were IgM positive, 106 patients were diagnosed with dengue fever, and 15 patients were in the severe critical phase of dengue infection. The distribution of patients according to serological tests and clinical manifestations is shown in Table 2.
Table 2 - Distribution of patients based on serological tests and clinical manifestations of Dengue
Dengue diagnosis tests | Number of patients | Percentage |
NS1 Positive | 212 | 35,33 |
IgM Positive | 155 | 25,83 |
Dengue fever | 106 | 17,67 |
Dengue-like illness | 126 | 21,0 |
Dengue critical phase | 15 | 2,50 |
Dengue Shock Syndrome | 10 | 1,67 |
Dengue Hepatitis | 4 | 0,67 |
Among severe complications, 10 patients developed dengue shock syndrome, of which four patients also had dengue hepatitis. Laboratory investigations revealed hematological abnormalities typical of dengue infection. Reduced RBC counts and hemoglobin levels below 9 g/dL were observed in several patients. A total of 84 patients had RBC counts below 4,5 million/cu mm, while 38% had leukopenia with WBC counts below 4000 cells/cu mm.
Platelet analysis showed that 120 patients had platelet counts below 100,000 cells/cu mm, and 86 patients had platelet counts between 51,000 and 100,000 cells/cu mm. Only four patients had platelet counts below 20,000 cells/cu mm, indicating very severe thrombocytopenia. Detailed hematological parameters are presented in Tables 3 and 4.
Table 3 - Variations in hematological parameters in dengue patients
Blood Counts | Normal range | Number of patients above the normal range | Number of patients below the normal range |
Hemoglobin | 13,5–17,5 gms/dl | 32 | 216 |
RBC | 4,50 to 5,90 Million/cu mm | 28 | 220 |
WBC | 4000–11000 cells/Cu mm | 50 | 198 |
Neutrophils | 40–75% | 162 | 86 |
Lymphocytes | 20–40% | 156 | 92 |
Esinophils | 1–6% | 58 | 190 |
Monocytes | 2–10% | 42 | 206 |
Table 4 - Variation in platelet counts of dengue patients and statistical analysisTa
Platelet Count Range (cells/cu mm) | Midpoint | n | % of 248 cases | Weighted Contribution |
<20,000 | 10,000 | 4 | 1,6% | 40,000 |
21,000–50,000 | 35,000 | 38 | 15,3% | 1,330,000 |
51,000–1,00,000 | 75,000 | 86 | 34,7% | 6,450,000 |
<1,00,000 (assumed 1,00,000) | 100,000 | 120 | 48,4% | 12,000,000 |
Total (n=248) | — | — | 100% | 19,820,000 |
Table 5 illustrates platelet count variation among dengue patients, demonstrating universal thrombocytopenia with a mean platelet count of 80,000 ± 25,000 cells/cu mm. Mild thrombocytopenia was observed in 48,4% of patients, moderate thrombocytopenia in 34,7%, severe thrombocytopenia in 15,3%, and very severe thrombocytopenia in 1,6%.
Regarding treatment practices, all patients (100%) received antipyretics, and 97,1% received intravenous fluids, reflecting the supportive management approach recommended for dengue. Antimicrobials were prescribed in 48,5% of patients, while antiemetics and antiulcer medications were used in 79,4% and 94,1% of patients, respectively. Intravenous fluid therapy is known to reduce dengue case fatality rates to approximately 1% in severe cases by correcting dehydration and preventing shock. Antipyretics and antiemetics were primarily used for symptomatic relief.
Antibiotics were administered mainly to patients with high neutrophil counts suggesting possible secondary bacterial infection or those presenting with severe clinical illness. Caripill (papaya leaf extract) was used in 68% of patients as a platelet supportive therapy, particularly in severe dengue cases. The overall prescribing patterns are summarized in Table 5.
Table 5 - Prescribing patterns
Drug class | Number of patients prescribed | Percentage of total, % |
Antipyretic | 270 | 45,0 |
IV fluids | 454 | 75,7 |
Antiemetic | 71 | 11,8 |
Antiulcer | 30 | 5,0 |
Antimicrobial | 125 | 20,8 |
Caripill | 18 | 3,0 |
4. Discussion
Dengue can present with a wide spectrum of clinical manifestations, ranging from asymptomatic infection to severe illness that may become fatal if not treated promptly. Early diagnosis and timely clinical management are therefore critical roles for healthcare professionals. Although many patients present only with the febrile phase, symptomatic dengue typically progresses through three phases: febrile, critical, and recovery. Predicting which patients will progress to the critical phase remains challenging. The present investigation assessed dengue prevalence in Mahabubnagar town along with prescribing patterns and treatment approaches used in clinical practice.
The study examined the prevalence of acute dengue virus (DENV) infection and factors associated with DENV positivity among rural and urban populations. Among the study participants, 48% were NS1-positive and 32% were IgM-positive, indicating active or recent dengue infection. Rural areas showed comparatively higher IgM and NS1 positivity than urban regions. Acute DENV infection was identified in 2,2% of participants, although no statistically significant difference was observed among the villages studied. These findings suggest that dengue infection has continued to persist and circulate in recent years. The higher prevalence among males aged below 20 years, followed by those aged 21–30 years, further supports the ongoing transmission of DENV infection in Mahabubnagar.
In the present study, most patients were males younger than 20 years, followed by individuals aged 21–30 years. This age distribution may reflect immunity patterns in the population, where older individuals may possess partial immunity due to previous exposure to dengue virus. Another explanation may be the increased outdoor exposure of younger individuals through college activities, social interaction, and recreational behavior. In semi-urban and rural areas of Mahabubnagar, male adults are commonly involved in agricultural and household work, particularly during early morning and late afternoon hours when Aedes aegypti mosquitoes are most active. Furthermore, awareness regarding personal protective measures such as wearing full-sleeved clothing, using mosquito repellents, and maintaining environmental sanitation remains limited. Similar demographic patterns have been reported in studies by Praful et al. , .
Dengue severity was evaluated using the dengue severity index score proposed by Surangrat et al., which integrates clinical manifestations and laboratory findings into a composite severity score. According to this classification, nearly two-thirds of patients in our study were categorized as severe dengue cases. This observation likely reflects the high-acuity nature of hospitalized patients included in the study population.
Seasonal variation in dengue incidence was analyzed using the Chi-Square test. The calculated Chi-Square statistic value (χ²) was 399,95 with 44 degrees of freedom, and the p-value was 6,47 × 10-59. As the p-value was extremely small, the results confirm a statistically significant seasonal variation in dengue incidence across the study period from 2019 to 2023. Although some months reported very few or zero cases, dengue incidence was not evenly distributed throughout the year. Instead, a clear seasonal pattern was observed, with higher case numbers during the post-monsoon months, particularly from September to November. The heatmap presented in Figure 1 visually illustrates these temporal trends. Across most years, especially 2019, 2020, and 2021, dengue cases peaked during September–November, reflecting post-monsoon increases in mosquito breeding. Conversely, the summer months from April to June showed relatively fewer cases, indicating less favorable conditions for dengue transmission. Interestingly, January 2020 recorded an unusually high number of cases (45) despite the pandemic period, followed by a sharp decline to zero cases. This unusual pattern may reflect changes in reporting systems or public health interventions during that time.
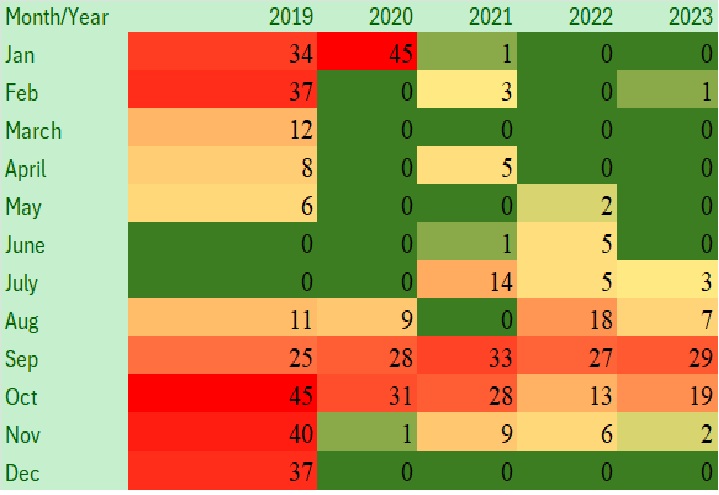
Heatmap: Seasonal Variation of Dengue Cases (2019–2023)
Regarding clinical manifestations, case reports from the study population indicated that the most common symptoms included headache, abdominal pain, myalgia, cough, cold, vomiting, and diarrhea. Dengue infection can affect individuals of all age groups; however, a considerable proportion of cases (48,31%) occurred among individuals younger than 20 years. Males accounted for 59,7% of the total cases. The mean age was similar across both sexes, and 48 patients (35,3%) demonstrated positive dengue serology.
Hematological alterations among dengue patients were analyzed in 248 out of 600 cases, as shown in Table 4. A large proportion of patients exhibited abnormal hematological parameters. Approximately 220 patients (88,7%) had RBC counts below the normal range, while 216 patients (87,1%) had reduced hemoglobin levels, suggesting anemia. These findings may reflect nutritional deficiencies or hemodilution occurring during the febrile phase of infection. Leukopenia was observed in 198 patients (79,8%), which is a typical laboratory feature of dengue infection. Viral infections such as dengue can lead to bone marrow suppression, immune-mediated destruction of white blood cells, and peripheral sequestration. Reduced eosinophil and monocyte counts were also observed, with 190 and 206 patients respectively showing values below the normal range. In contrast, neutrophil and lymphocyte counts were elevated in some patients, possibly reflecting different stages of disease progression. Overall, the hematological profile observed in this study—characterized by leukopenia, low hemoglobin, reduced RBC counts, and decreased eosinophil and monocyte levels—was consistent with classical laboratory findings reported in dengue patients. Similar hematological changes have been reported in previous studies , , which also documented significant reductions in RBC, hemoglobin, and WBC counts.
Platelet count analysis among the same cohort (248 out of 600 cases) demonstrated that all patients had platelet counts below 1,50,000 cells/cu mm, indicating thrombocytopenia as a common clinical feature of dengue infection (Table 5). Nearly 48,4% of patients exhibited mild thrombocytopenia, which is typically observed during the early febrile phase. Approximately 34,7% of patients showed progressive platelet decline associated with the transition toward the critical phase of dengue infection, where the risk of plasma leakage increases. Severe thrombocytopenia was noted in 15.3% of patients and was associated with hemorrhagic manifestations of dengue. A small proportion (1,6%) experienced extremely severe thrombocytopenia, indicative of dengue hemorrhagic fever or dengue shock syndrome, conditions that require close monitoring and may necessitate platelet transfusion.
The treatment modalities observed in this study were largely consistent with the WHO and Indian national dengue management guidelines. With the increasing frequency of dengue outbreaks, adherence to standardized treatment protocols has become essential to ensure optimal patient outcomes.
Antimicrobial utilization was observed in approximately 48.5% of cases. Most medications prescribed were approved by regulatory authorities and included in essential medicines lists, supporting rational prescribing practices. However, the use of antibiotics in dengue patients likely reflects clinical concern about potential secondary bacterial infections. Since dengue is primarily a viral disease, such antibiotic use also raises important considerations regarding antimicrobial stewardship.
Another notable finding was the frequent use of Caripill (papaya leaf extract) for managing dengue-related thrombocytopenia, with 68% of patients receiving this therapy. This observation highlights the increasing interest in natural or supportive treatments in dengue management. Some studies have suggested that papaya leaf extract may help improve platelet counts in dengue patients . However, its use has not yet been formally included in treatment guidelines issued by organizations such as the WHO. Further well-designed clinical trials are required to establish its safety and effectiveness, particularly in pediatric populations. If proven beneficial, papaya leaf extract could become a cost-effective supportive therapy, especially in resource-limited healthcare settings.
The increasing number of dengue cases, particularly during post-monsoon months, underscores the need for targeted seasonal vector control strategies. Similar seasonal patterns have been reported in other regions of India, where dengue incidence peaks between August and November due to favorable mosquito breeding conditions following rainfall , . The higher number of cases observed in rural areas in the present study may be associated with poor sanitation, stagnant water accumulation, and limited access to preventive healthcare services. These factors have also been highlighted in previous studies . Therefore, strengthening community awareness, improving waste management practices, and implementing effective mosquito control measures by local authorities are essential to reduce dengue transmission, particularly in vulnerable rural communities.
This retrospective study had several limitations. First, the study was restricted to Mahabubnagar district, which may limit the generalizability of the findings to other regions of Telangana. Second, hematological data were missing in some cases, which may have affected the interpretation of laboratory trends. Third, as the study relied on hospital records, it may not have captured dengue cases occurring at the community level or those managed outside tertiary care hospitals. Finally, the assessment of prescribing patterns was based solely on hospital documentation and did not evaluate patient adherence or clinical outcomes. Despite these limitations, the study provides valuable insights into dengue prevalence, hematological patterns, and treatment practices in Mahabubnagar district of Telangana. These findings highlight the need for region-specific surveillance systems, improved vector control strategies, and optimized treatment approaches for effective dengue management.
5. Conclusion
Dengue continues to pose a significant health challenge in Mahabubnagar, with a clear seasonal trend and high rural burden. While symptomatic management remains the cornerstone of treatment, there is an urgent need for preventive strategies, including public awareness, environmental sanitation, and evidence-based supportive therapies. Policymakers and healthcare providers must collaborate to develop effective surveillance, preventive, and therapeutic frameworks tailored to regional realities.